
Inflammatory Bowel Disease (IBD) is a chronic condition that includes Crohn’s disease and ulcerative colitis. Symptoms are often invisible and unpredictable, making it difficult for clinicians and patients to understand what’s happening inside the bowel. Imaging plays a central role in diagnosis and monitoring, but traditional methods can be subjective, time-consuming, and invasive.
IBD assessment is complex for both clinicians and researchers.
Patients may feel unwell despite limited visible inflammation, or conversely, feel fine while inflammation persists. This mismatch makes symptoms alone an unreliable measure.
While colonoscopy and biopsy remain gold standards, they are uncomfortable, costly, and only examine limited bowel regions. They are also prone to inter-observer variation.
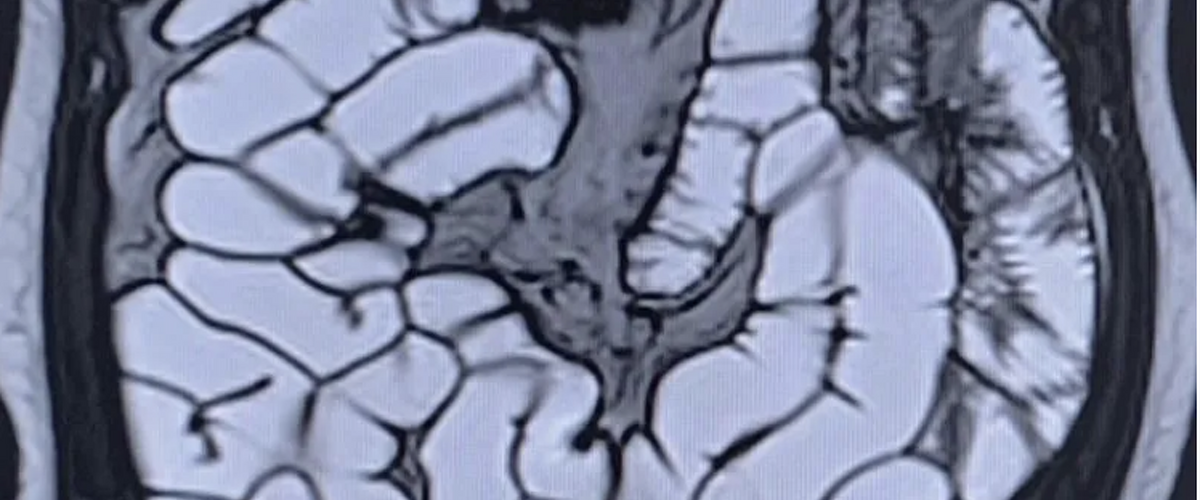
MRI and intestinal ultrasound are increasingly used for whole-bowel assessment, but cine loops and dynamic scans can be time-consuming to review and difficult to standardise.
Capsule endoscopy and histopathology provide valuable information, but data are hard to integrate with imaging and clinical findings.
Variability in how images and biopsies are interpreted makes it difficult to run efficient multi-centre trials. Consistent biomarkers are needed to support regulatory acceptance.
Patient-reported outcomes (PROs) are critical for understanding real-life disease burden, but collection and integration remain inconsistent.
Together, these approaches make IBD assessment more transparent, reproducible, and meaningful - for clinicians, researchers, and patients.
Motilent is transforming how IBD is measured, monitored, and understood - across clinical care, research, and patient engagement.
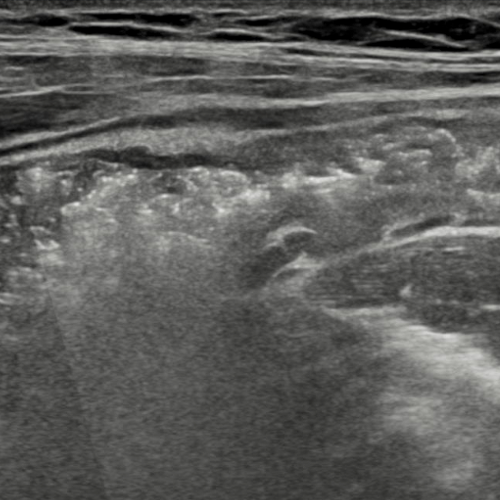
A secure solution for capturing, storing, and sharing intestinal ultrasound (IUS) data.
Learn more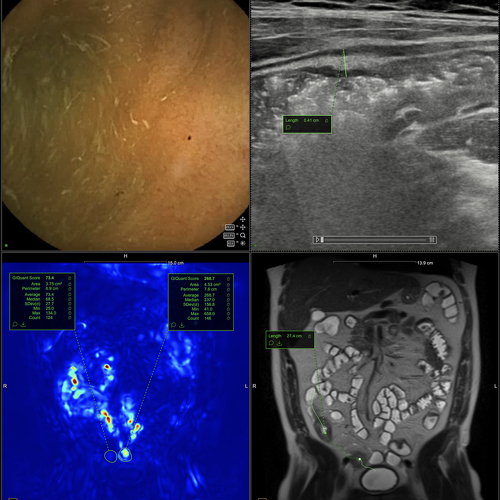
Motilent's secure, cloud-based platform, optimised for gastrointestinal data.
Learn moreAssesses small bowel motility, producing an objective score to support Crohn’s disease activity monitoring
Learn more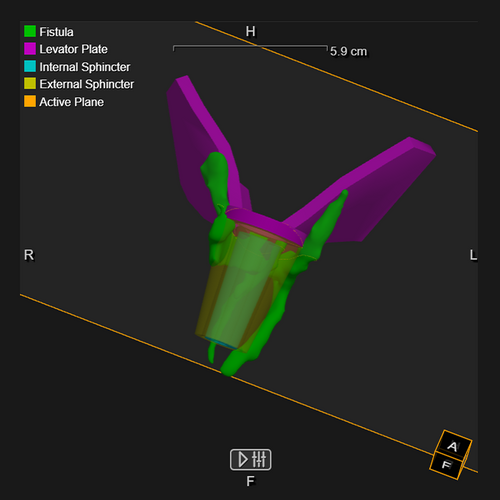
Multiple peer-reviewed studies show that small bowel motility measured with GIQuant correlates with inflammation and treatment response in Crohn’s disease.
GIQuant has been adopted as an imaging endpoint in multi-centre Crohn’s disease trials, supporting objective and reproducible outcome measures for regulatory submission.
Motilent is exploring integration of MRI, intestinal ultrasound, capsule endoscopy, and histopathology, as well as patient-reported outcomes via IBDmate, to create a more comprehensive understanding of IBD activity.
Get in touch to discuss how Motilent can support your IBD practice, research study, or clinical trial.